A Collaboration with: William “Sandy” Wells, and Eric Halgren
This translational research project combines preoperative high-resolution functional MRI (fMRI) with intraoperative electrophysiologic testing (ECS) in patients with low grade brain tumors in eloquent motor and language cortex in order to accomplish the following general goals:
- understand the relationship between the fMRI signal and neuronal activity;
- develop methods which will improve fidelity of preoperative functional brain mapping;
- improve outcomes for patients with tumors in and around motor and language cortices; and
- accurately assess the validity of this approach.
Since its early development, there has been tremendous enthusiasm for the potential of fMRI as a clinical tool, especially for functional mapping for brain surgery. fMRI at high field strengths has an excellent signal-to-noise ratio (SNR) and high spatial resolution and is able to demonstrate task-associated brain activity in single subjects. fMRI is non-invasive, does not require exposure to ionizing radiation, and can be readily repeated to follow clinical changes.
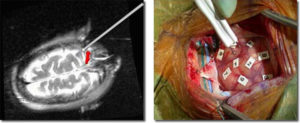
Intraoperative use at BWH of fMRI and ECS brain mapping for localization of eloquent cortex. (left) Intra-operative imaging demonstrates coregistration of preoperative fMRI motor mapping data (red) with updated MR image of brain and probe position (right) Intra-operative photograph showing electrical cortical stimulation mapping with markers indicating areas which have been tested.
In general, while basic cognitive scientists have used fMRI to investigate the brain-basis of specific cognitive processes, there has been little direct validation of these findings with electro-cortical recording from the brain. Additionally, in order for fMRI and other non-invasive brain mapping techniques to be useful for clinical neurosurgical planning, they must be validated against the gold-standard of intraoperative ECS. While there has been some fairly gross validation of basic motor and language function, there has not yet been any fine quantitative comparison between these methods in humans. There are multiple factors contributing to the difficulty of making pre-operative fMRI a reliable, valid and useful method for the determination of eloquent cortex. To date, pre-surgical fMRI studies have had a fairly gross spatial resolution. This, in addition to issues relating to the selection of a statistical threshold, makes determining the limits of activation problematic. If fMRI is to become a tool with sufficient sensitivity to be predictive of clinical outcomes it must provide information that is at least as spatially precise as the ECS standard. A second significant obstacle to accurately and quantitatively comparing fMRI and ECS is the difficulty of accurately coregistering fMRI data to intraoperative brain anatomy. Another difficulty involves the uncertainty about what the relationship of areas of activation in fMRI is to areas which show disruption of function during ECS. Finally, there is little current knowledge of how the electrical current introduced during ECS propagates through the cortex, nor is there a complete understanding of the neuronal response to cortical stimulation.
In order to improve pre-operative functional mapping and to better understand the relationship between fMRI-demonstrated activation and intraoperative determi, this collaborative research project will bring together researchers from various fields to:
- Develop reproducible behavioral paradigms;
- Develop high-resolution techniques for presurgical fMRI acquisition and analysis;
- Mathematically model electrical stimulation current in the cortex during ECS;
- Use laminar electrodes to record from the cortex around stimulation sites to measure current spread and neuronal response;
- Accurately coregister data sets from fMRI and ECS to intraoperative anatomic MR images;
- Statistically compare results obtained from fMRI and ECS.
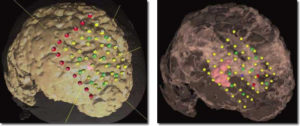
(left) Intra-operative neuronavigation GE InstaTrak screenshot: right-frontal mass lesion (pink); 6×8-electrode grid with 35 electrodes within the craniotomy (yellow dots) and 13 electrodes outside the craniotomy (red dots). (right) 3D Slicer software screenshots for off-line comparative analysis of intraoperative ECS motor testing sites and preoperative fMRI motor function: right-frontal mass lesion (pink); fMRI activation (blue); electrode strips (yellow dots); negative ECS sites (green dots); and positive ECS sites (red dots).